  |
 |
 |
 |
 |
|
|
|
|
|
Lab 10, Page 4 of 43
This nerve is considered to contain only motor fibers innervating the muscles of the tongue.
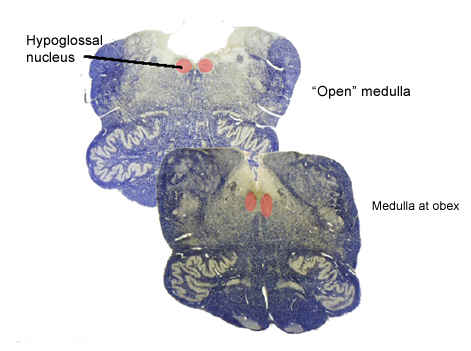 The hypoglossal nucleus contains the cell bodies of the axons that innervate the tongue musculature. Damage to the hypoglossal motor neurons results in a flaccid paralysis and atrophy of the ipsilateral tongue and in the deviation of the tongue towards the side of the lesion during protrusion of the tongue (paralysis of the genioglossus muscle).
The hypoglossal nucleus contains the cell bodies of the axons that innervate the tongue musculature. Damage to the hypoglossal motor neurons results in a flaccid paralysis and atrophy of the ipsilateral tongue and in the deviation of the tongue towards the side of the lesion during protrusion of the tongue (paralysis of the genioglossus muscle).
The somatosensory systems of the face area (i.e., the trigeminal sensory nuclei) provide direct and indirect (via the reticular formation) input to the hypoglossal nucleus which mediate reflex tongue movements in response to stimuli from lingual, oral and pharyngeal mucous membranes.
The cortical input to the hypoglossal nucleus is bilateral with a slight contralateral dominance and both direct and indirect. Bilateral damage to the corticobulbar tracts results in motor defects called the pseudobulbar palsy syndrome. Voluntary movements of the tongue are greatly impaired and speech is quite dysarthric. Muscle atrophy does not usually occur and this serves to differentiate the type of paralysis and aids in localizing the lesion. Other types of cranial motor disorders that appear in the pseudobulbar palsy syndrome depend upon the level of involvement of the corticofugal fibers. Damage to the basal ganglia may cause involuntary, irregular movements of the tongue.
Clinical Testing of Cranial Nerve XII:
Go to the NEXT PAGE
